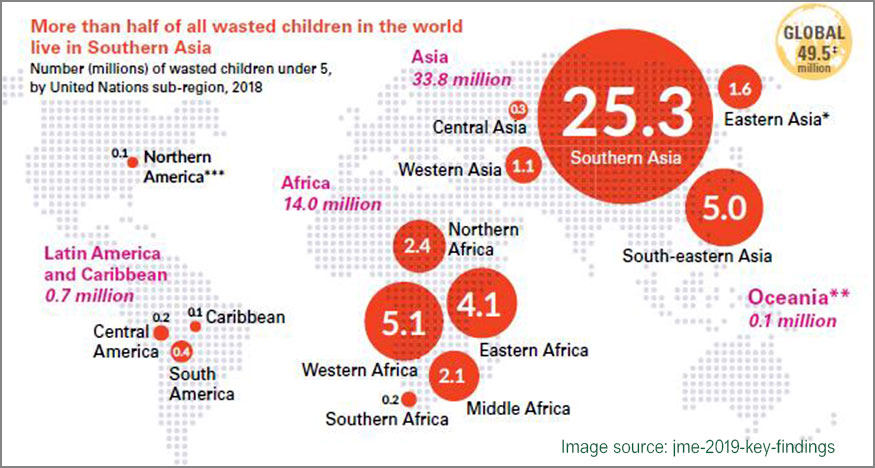
South Asia accounts for more than 25 million (approx.) wasted children in the under-five age group, with 4 out of 5 such children residing in India. Such a heavy burden, coupled with the absence of any effective, long-term health program specific to Severe Acute Malnutrition(SAM) has put the entire health setup in dire straits, unequipped to deal with pressing health issues of the present and future effects. Since the prevalence of SAM is much more prominent during the initial 6 months of a child’s birth, it contributes to high mortality rates in U5 group if not treated on priority. Given that burden of SAM-afflicted children is disproportionately high as compared to the institutional facilities and their respective capabilities, it thus becomes indispensable to adopt a streamlined community-based approach to change the current trajectory of SAM pathway in India for good. Though treatment of SAM has undergone a paradigm shift over the past decade through advocacy and promotion of CMAM approach (Community-based Management of Acute Malnutrition), India still has not embraced CMAM wholeheartedly.
National Family Health Survey (NFHS-4, 2015-16) data presents a bleak scenario regarding SAM statistics, and how it has progressively worsened over time. The proportion of U5 children suffering from severe wasting showed an increase from 6.4% in 2005-06 to 7.5% in 2015-16. Those in the category of wasting increased to 21% (2015-16) from 19.8% (2005-06). Rise in SAM prevalence despite a multitude of efforts by all stakeholders shows its deep entrenchment in Indian society. Redressing the situation calls for a radical change in the way we view malnourishment treatment through instilling care practices consistent with the preventive and curative methodologies essential for handling SAM better.
According to the WHO guidelines about best practices to deal with SAM, a synergised action at institutional and community level is essential to deal with SAM effectively. This integrated multi-sectoral synergised approach could comprise of in-facility treatment of children afflicted with illnesses, and out-patient management of children without medical complications in community settings using Ready-to-Use Therapeutic Food (RUTF).
As a principle, CMAM focuses on both treatments as well as prevention of future SAM cases which brings down the incident burden. This provides a great opportunity to eradicate SAM from the target populace if implemented rigorously. CMAM entails significant mortality reductions in varied national settings, which means that a comprehensive response to severe wasting in children is not possible without including CMAM firmly on the agenda. Since the incidence of wasting is highest at birth (37%), nutrition-specific interventions like RUTF can be made available under the overarching ICDS Scheme.
In India, the CMAM approach was implemented during 2009 Kosi floods by MSF and a cure rate of 89% was achieved, along with reduced mortality rates. A dozen other pilots in states all over India has generated enough evidence for moving away from a Facility-based SAM (F-SAM)-only model to treating children with no medical complications in Nutrition Rehabilitation Centres (NRCs), on the lines of POSHAN Abhiyaan by the Rajasthan government. This will enable developing a holistic solution to a teething public health concern needing immediate attention. Better recovery rates for children have been observed when children are administered RUTF/nutrient-dense foods instead of solely depending on F-SAM. When implemented at a large scale, this could prove to be the ultimate panacea for children in urgent need of care.
Reference:
-
- https://www.ennonline.net/fex/60/continuumofcareindia?version=current
- https://www.indianpediatrics.net/oct2017/oct-813-814.htm
- https://www.ncbi.nlm.nih.gov/books/NBK361900/
- http://www.who.int/nutrition/topics/globaltargets_wasting_policybrief.pdf
- https://www.msjonline.org/index.php/ijrms/article/download/4958/4373